
Understanding Arousal: The Mind–Body Connection in Sexual Wellbeing
Sexual arousal can be surprising for many in the way it operates, sometimes leading to confusion of frustrating. This blog will firstly define what arousal is, and introduce how the brain coordinates your sexual response. You’ll learn how multiple factors shape your experience of sexuality, debunk myths, explore practical steps today, and how sex therapy can provide support.
Why Can’t I Get Turned On?
Prefer to listen? In this podcast I explore arousal, answering the question, “Why can’t I get turned on?”
What Is Arousal?
Sexual arousal is the readiness of mind and body for sexual activity. It is both a psychological and physiological process.
Physiological changes to the body:
When sexual arousal occurs, your whole body experiences changes such as increased muscle tension, heart rate, and awareness of pleasurable sensations.
Physiological changes to the Vulva:
- There is an increase in blood flow to the vagina and vulva
- This results in clitoral swelling, the swelling and darkening of the labia minora (inner lips of the vulva)
- Vaginal blood flows allows for vaginal lubrication
- Other changes to a female body include the elevation of the uterus, enlargement of breasts, and erect nipples
Physiological changes to the Penis:
- The smooth muscles of the penis relax, allowing blood flow into the penis, which causes an erection
- The testes swell and elevate
- Precum may be secreted
When the mind experiences arousal, this may be experienced as being “turned on”, excited, or “ready” for sex.
Pathways to Arousal
The body’s capacity for arousal relies on your brain and your spinal cord. It is the coordination of this complex communication network that results in blood flow and genital swelling. There are two main bodily pathways for sexual arousal signals to travel through: the head route, and the touch route.
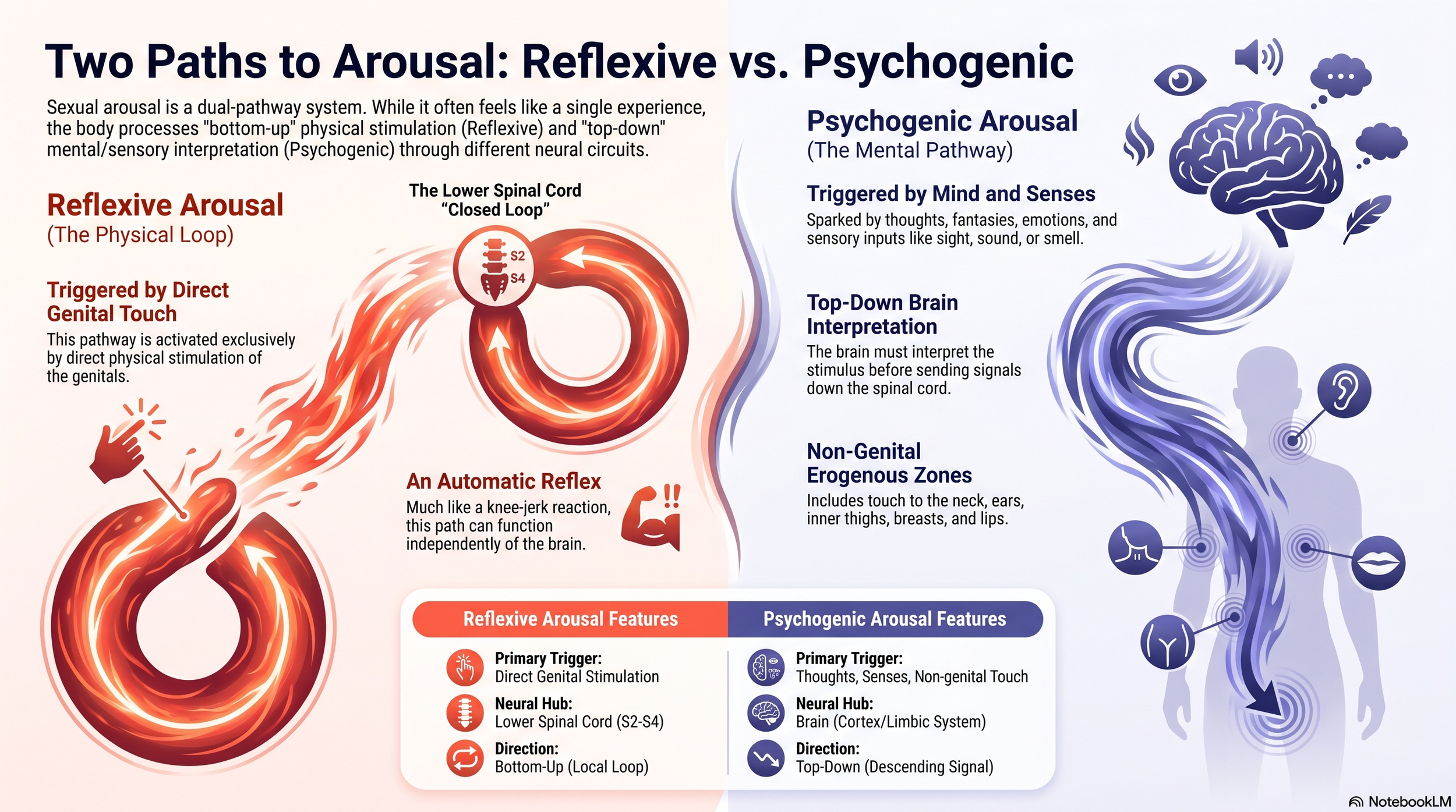
The mind and body pathways to arousal.
The head route (psychogenic arousal):
This pathway is triggered by the mind through thoughts, emotions, memories, fantasy, and sexual stimuli. Your brain’s cerebral cortex which is responsible for higher mental processes, digests this information and sends signals down your spinal cord. The head route explains how visual stimuli, thoughts, sounds, and even smells can “turn you on”. Touch to sensitive areas such as the nipples, breasts, lips, mouth, inner thighs, neck, and earlobes are processed by the brain to also create arousal.
The brain is the body’s most important sexual organ, and this is displayed in the ability for individuals to experience orgasm without physical genital contact. Purely through sexual thought, fantasy, dreams, psychogenic arousal can be stimulated powerfully enough for orgasm to occur.
The touch route (reflexive arousal):
This pathway is triggered by direct physical touch to and stimulation of the genitals.
Direct stimulation of the genitals trigger signals to the lower spinal cord which then sets of a reflex action of genital arousal. This reflex is involuntary and automatic, similar to a knee jerk reaction. This pathway of arousal becomes especially important with age. Due to changes in the body, over time, the head route also needs the touch route to experience full arousal.
Integrating head and touch pathways:
Both pathways matter for the full experience of sexual arousal, and the pathways are deeply connected. The brain is always influencing the body through its interpretation and meaning making of touch. Even when the spinal cord is receiving touch signals from physical touch, the mind can block the physical response if it is experiencing fear, anxiety, or stress. Physical changes can also influence the brain, for example touch opening up the touch route, being perceived as pleasurable, then leading to sexual thoughts, opening up the head route, and contributing to more physical arousal.
Sometimes one pathway is stronger than the other, or one route can be weaker. Understanding how your pathway works can help you to maximise your arousal. For example, there may be a lack of strong tactile sensation, but you are able to cultivate arousal through intentional sexual thoughts or using your mind to zone in on sensory awareness.
It is also important to recognise that sometimes the body can respond with arousal signs such as lubrication, even when the mind remains neutral or switched off. This is the experience of “nonconcordance” where there is a mismatch between physical arousal and mind arousal. The arousal of the mind is very subjective, and in these instances matter more than the physical arousal. Just because an individual may experience physical arousal, does not automatically mean they are ready for, or excited for sex. This is one reason why physical arousal alone should never be assumed to indicate desire, enjoyment, or consent.
Nonconcordance can also occur when one is mentally turned on but does not experience genital arousal. It may be there are psychological road-blocks that complicate the mind-body feedback loop, or complications caused by physical factors such as changes simply due to ageing, or sometimes serious physical health issues such as chronic illness, disease, or injuries.
While the head route and the touch route to arousal, explain the pathways to arousal, the Dual Control Model governs these pathways, much like traffic lights giving the green light to arousal, the yellow light slowing arousal down, or the red light which halts arousal altogether.
The accelerator and brakes of arousal: The Dual Control Model
There are two distinct systems in the brain that control arousal, the Sexual Excitation System (SES) and the Sexual Inhibition System (SIS).
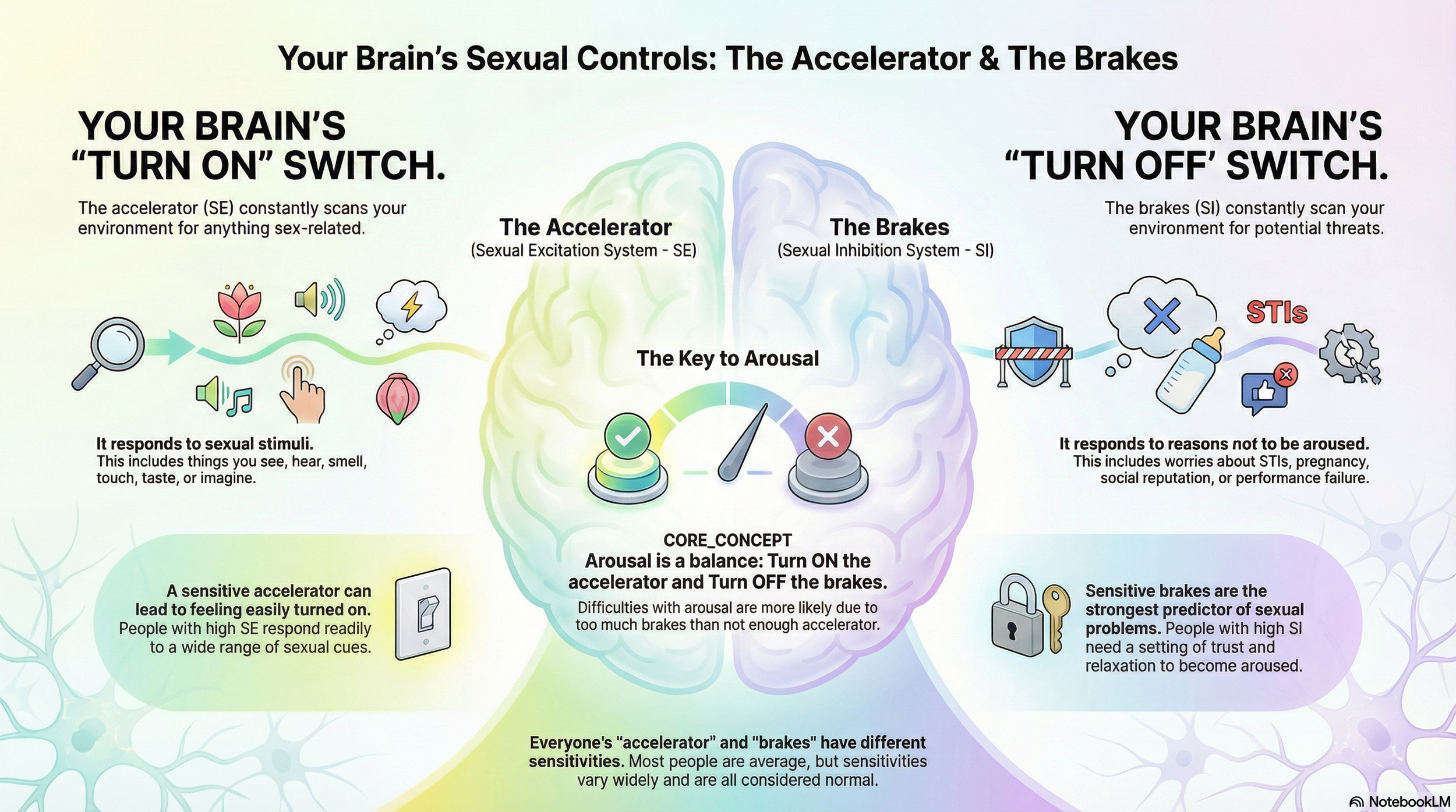
The dual control model of sexual arousal: learning to turn on the on, and turn off the off.
The SES is the accelarator to arousal. When activated it is responding to anything the brain perceives as sexually relevant. This could be sexual thoughts, physical touch, seeing an attractive person, your partner’s behaviours, and even internal feelings and sensations.
The SIS is the brakes to arousal. It activates to anything the brain perceives as a reason not be sexual right nor such as threat, danger, worry, stress, disinterest, timing etc
Another way to think of it is the SES is an accelerator that makes the car of arousal drive, and the SIS is the brakes. For the car to drive, the accelerator (SES) must be activated and at the same time the brakes (SIS) must be released. Pressing the accelerator harder will make the car go nowhere, so long as the brakes are activated.
Individuals uniquely experience SES and SIS. One system may be more sensitive than the other. This is not right or wrong, just different. However, it is important to consider what turns you “on” AND what turns you “off”. Until what turns you “off” is addressed, even with a sensitive accelerator, the car of arousal will go nowhere.
This system interacts with the head and touch pathways. For example, you might experience sexual thoughts about your partner (head pathway), but because you feel smelly after a run (hitting the brakes/SIS), do not feel arousal or readiness for sexual activity. For another person entirely, this same situation may not hit the brakes at all, in fact feeling good and strong in your body after a run, despite the smell may hit the accelerators. Another example is your partner cheekily gropes you on your backside (touch pathway), but you’ve just had an argument (hitting the brakes/SIS), and this is a complete turn off, and in fact, makes you more pissed off. And yet for another person, this same act might hit the accelerator, because they enjoy make-up sex.
Desire vs Arousal: What’s the Difference?
Desire and arousal are terms that are often used interchangeable, however these are distinct terms. At the same time, there is significant overlap between these concepts, which is why they are often confused.
Desire is the motivation, thinking about/wanting to have sex, sexual thoughts or fantasy, urge to engage in sexual activity.
Sexual arousal is when the body and mind is prepared for or ready for sex.
Desire and arousal can occur at the same time, sometimes desire leads to arousal, and sometimes arousal leads to desire.
Common Factors That Influence Arousal
1. Physical factors:
Chronic illnesses and medication side effects contribute to many physical sexual problems such as erectile dysfunction. Read about ED here.
Testosterone is a crucial hormone for desire in all individuals, which also influences arousal
Ageing and the natural changes that occur in the body mean that arousal often takes more time due to system efficiency. Read about changes to the vulva here, and changes to the penis here.
Fatigue and a lack of sleep can also significantly impact arousability, due to the natural wear and tear of the body
2. Psychological factors:
Anxiety and performance pressure for most people hit the SIS/brakes, as this activates the body’s fight or flight system of protection from threat. Arousal most often requires relaxation.
Spectatoring is the experience of “watching” yourself or monitoring yourself during sex, which is a huge distraction away from sensation and pleasure
Depression, anger, stress, and shame can negatively impact arousal and desire
Past trauma can condition the brain and body to broadly interpret sexual situations both safe and unsafe as threats, inhibiting arousal
Individuals with a sense of believing they are worthy of pleasure, strong self-esteem, and accepting of their body, often experience greater sexual satisfaction
3. Relational factors:
The quality of your relationship including feelings of trust, connection, and affection can impact significantly on arousal. For many people, it is the relationship that helps to hit the accelerator, and for many relational discord can hit the brakes to arousal.
Everyday communication AND the ability to communicate sexually is important. Healthy communication is the scaffolding of an intimate, connected relationship. Likewise, communicating positively about sex can increase sexual satisfaction.
A partner’s overall health and sexual health, especially when this is taken personally or where one partner becomes a caregiver rather than a supportive partner, can negatively impact arousal.
4. Environmental/contextual factors:
Everyday stressors such as household responsibilities, finances, and parenting can both reduce time for sexual intimacy, but also mental, emotional, and physical bandwidth for sexual intimacy.
Sex that is a chore or a responsibility, becomes another task on the never-ending to-do list, and is not particularly sexy- dampening arousal.
Messages derived from society, family, and friends can reinforce unhelpful but deeply held beliefs about sex that impact on arousability.
Myths About Arousal
Physical arousal proves arousal, desire, or consent. Genital changes can be a reflexive response to stimuli, and do not automatically mean liking, wanting, or a consent to sexual activity. It is important to take into an account a person’s body, behaviour, AND words. One can be physically aroused and not want to have sex. The reverse is true – where one may want to have sex, but have difficulties with physical arousal.
If you need lube, you are not aroused enough. Lubrication in the vagina is a sign of physical arousal. Mental arousal can also trigger physical arousal and vaginal lubrication. At the same time, additional lubrication is needed by many women, especially with age or prolonged stimulation. Lubrication is a great enhancer of arousal, comfort and pleasure. Read the blog on changes to the vulva here.
If a penis loses its erection, you’re not aroused enough. While it is true that there may be mental factors hitting the brake on arousal, which impacts erection, this is not always the case. What is guaranteed however, is worrying about your erection, or shaming yourself after loss of an erection, is a sure-fire way to hit the arousal brakes (from on to off, or further off if they were already pressed). It is possible to be mentally aroused, but naturally fatigue physically and experience lessened physical signs of arousal, especially with age. If mental arousal and desire is still there, one can flexibly explore other forms of intimacy, rather than taking this as a sign to stop being intimate, which unhelpfully reinforces performance pressure. Read the blog on changes to the penis here.
The whole point of sex is penetration leading to orgasm. This script often contributes to sexual dysfunction, rather than sexual satisfaction. This myth often drives performance driven sex, which then creates performance anxiety. Sexual satisfaction is measured by pleasure, which can include orgasms and intercourse, but not always. Pleasure can be derived from the many forms on sexual intimacy, including but not limited to intercourse.
Practical Steps You Can Try Now
Identify what turns you on and what turns you off. Strategically reduce known brakes and incorporate more accelerators.
Identify which pathways are strongest for you- is it the head or physical pathway? How do these pathways interact for you? How can you incorporate more of this with partner sensuality?
Communicate with your partner your above reflections. Treat your sexual intimacy as a team effort and exploration into pleasure.
When to Seek Support
· If arousal difficulties cause significant distress to you or your partner
· If you have attempted to improve sexual intimacy, but the problem has not changed or worsened
· If you and your partner are caught in a pattern of sexual avoidance or sexual obligation
· If you believe physical causes may be underlying arousal difficulties (seek out your GP as a first step!)
· If past trauma (including but not limited to sexual trauma) is impacting on your sexual wellbeing.
How Sex Therapy Can Help
Sex therapy offers a space to understand how the body, mind, and emotions interact to shape arousal. While medical care can explore physical causes, therapy focuses on the psychological, relational, and contextual factors that influence your sexual response.
In therapy, we unpack the unique factors that “press your brakes” or “release your accelerators.” This might include anxiety, shame, stress, body image, or relationship dynamics. Together, we explore ways to reduce inhibition, strengthen emotional and physical safety, and foster curiosity rather than performance pressure.
Therapy helps you rebuild trust in your body, learn how to tune into sensation, and identify what supports your arousal. For couples, sex therapy can help improve communication, deepen emotional intimacy, and develop teamwork around sexual exploration rather than focusing on performance or “getting it right.”
The goal of sex therapy is not to create constant or perfect arousal but to cultivate comfort, confidence, and connection in your body. By understanding how your unique arousal system works, you can move toward a more fulfilling, responsive, and pleasurable sexual experience.
Final Reflection
Arousal is a living process that responds to context, emotion, and connection. Everyone’s arousal patterns are different, and changes over time are normal. When we let go of performance expectations and learn to understand our body’s signals, sexual intimacy can become more authentic, flexible, and satisfying.
If you’re feeling stuck, disconnected, or anxious about your arousal, you don’t have to navigate this alone. With the right support, you can rediscover confidence, pleasure, and connection with yourself and your partner.
I offer online sex therapy across Australia, providing a safe and confidential space to explore these experiences and support your sexual wellbeing.
Written by Justine
References:
Gambescia N, Weeks GR, Hertlein KM. A clinician's cuide to systemic sex therapy. . 3rd ed. New York Routledge; 2021.
Nagoski E. Come as you are: the surprising new science that will transform your sex life. Simon & Schuster trade paperback edition, revised and updated. New York: Simon & Schuster Paperbacks; 2021.
Lambert D, Quicke J. Female arousal and orgasm. Singapore: Bentham Science Publishers Pte. Ltd.; 2023.
Kaplan HS. The new sex therapy: active treatment of sexual dysfunctions. New York: Routledge; 2011.
Lehmiller JJ. The psychology of human sexuality. 3rd ed. [Location Unknown]: John Wiley & Sons Ltd.; 2024.