
Premature Ejaculation Treatment Options
How to Stop Premature Ejaculation?
Premature ejaculation (PE) is the most common sexual dysfunction for men. To get a basic understanding of PE: what it is and causes, read my blog here.
If you think you are struggling with PE, or simply concerned about penis function, it is important as a first step to consult with your doctor/GP.
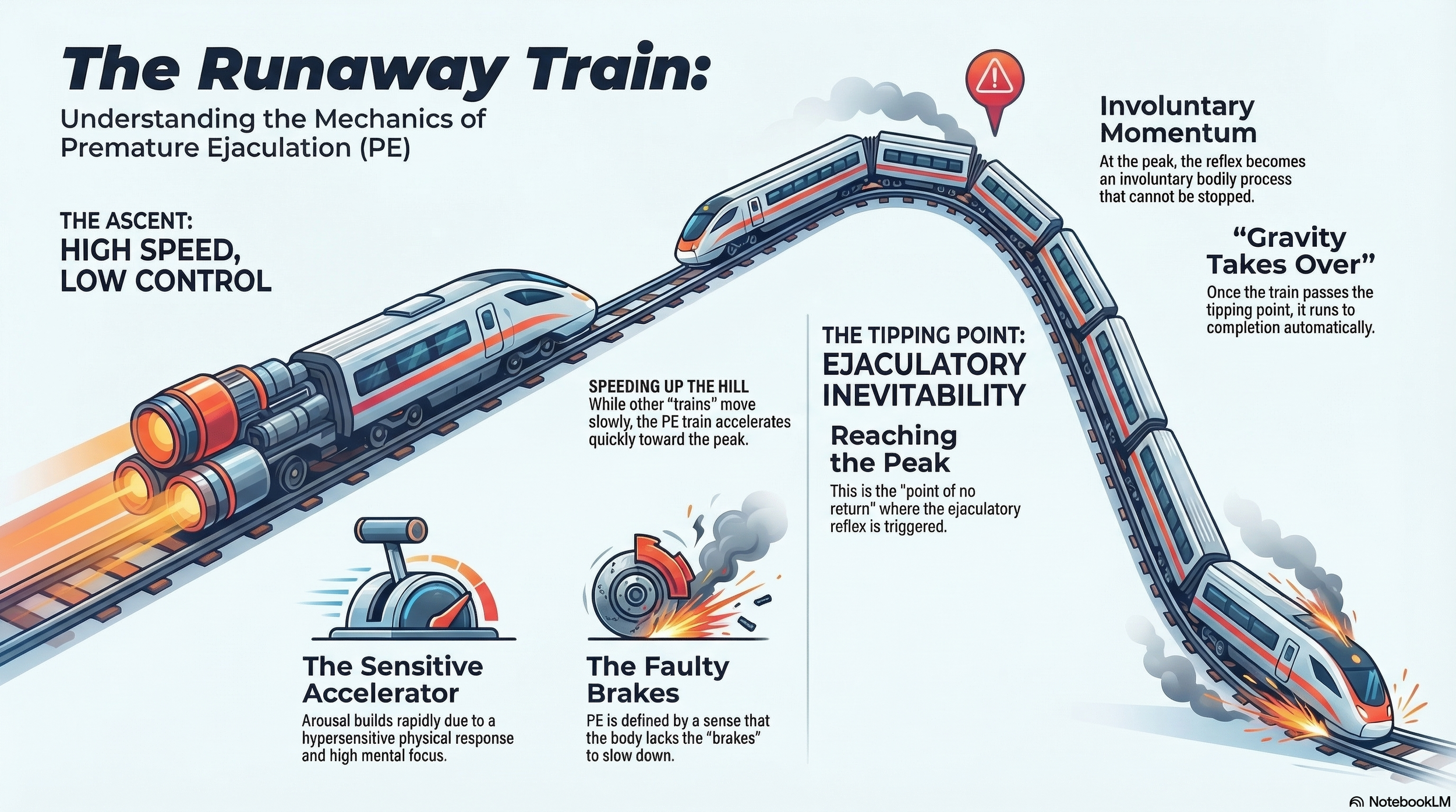
A helpful metaphor to understand PE is the concept of the runaway train. Imagine a train with a highly sensitive accelerator and faulty brakes. It is travelling up a hill with everything thrown onto the accelerator, at full speed. While other trains might travel more slowly up the hill: a person with PE’s train speeds up that hill much faster due to a combination of sensitive acceleration and the sense that everything is pressing the accelerator. Then as it reaches the peak, the tipping point (ejaculatory inevitability), the train loses control. At this point, gravity takes over and there is no stopping the train. This is true of all “trains” when they reach that tipping point; it is an involuntary, bodily reflex. The challenge for PE is that the train speeds up the hill too quickly, without any sense of control, and the inability to brake.
Sensitive accelerators and faulty brakes may be due to a combination of biological, psychological, and behavioural conditioning factors. Accelerators can include anxiety, which can activate the body’s fight or flight system. This can prime and rush the ejaculatory reflex, like pouring rocket fuel into the engine. (Interestingly this can have the opposite effect on others and is a major factor in Erectile Dysfunction). At the same time, the brake is underperforming, which in some cases may be due to reduced levels of the neurotransmitter serotonin which regulates ejaculation.
Premature Ejaculation, speeding up the hill too fast.
In this blog we will explore the treatment options for PE and the pros and cons of each option.
Can Premature Ejaculation Be Cured?
PE is highly manageable and treatable with the right supports. It is important to consult with a professional to explore important factors such as whether PE is lifelong or aquired, and underlying causes. These factors are important to consider in the treatment of PE. The treatment of PE becomes more effective when we understand exactly what it is we are treating (the causes).
Behavioural techniques: this includes the “stop-start” technique, the “squeeze” technique, and sensation awareness exercises. These exercises teach men to pay attention to and understand their levels of awareness and gain voluntary control over their ejaculatory reflex.
It is important to note that these techniques are best explored within the context of Sex Therapy which can explore the couple dynamics, address and manage couple anxiety or performance pressure.
Linking this in with the train metaphor, behavioural techniques are like driver’s education. They teach the driver to read the train’s dashboard and recognise when and how to ease off the accelerator and tap the braked, before reaching the top of the hill.
Pros:
- Improves overall sexual satisfaction and intimacy for both partners
- These techniques are permanently a resource once learned
- Physically safe
- The psychological and relational factors that contribute to PE are directly targeted
Cons:
- Often highly dependant on the cooperation and support of the sexual partner
- Long-term success rates can wane after a year, especially when exercises are not practiced consistently
- Time, money, and commitment required when combined with Sex Therapy
Topical Anaesthetic Agents:
Please note it is important to seek medical advice and prescription before using these methods. This includes prescribed creams (EMLA) and sprays (TEMPE) which mildly numb the penis and reduce sensitivity. These are generally applied to the head of the penis, 5-30 minutes before intercourse. These anaesthetic agents typically contain lidocaine and prilocaine.
By reducing sensitivity, topical agents can act as a speed governor on the train’s accelerator, slowing things down. This way the train moves up the hill at a much slower, manageable pace.
Pros:
- Highly effective at delaying ejaculation
- Compared to oral medications there are minimal bodily side effects
- Newer formulations are easier to use and act quickly and do not need a condom (TEMPE spray)
Cons:
- May cause loss of sensation to the penis, burning, or loss of erection
- They can be messy to apply
- Require anticipation of sex
- A condom is required to prevent transfer to a partner which can cause vaginal numbness, burning, or lack of orgasm
Daily Oral Medications:
Again, any medication requires prescription.
Due to serotonins role in the ejaculatory reflex, selective serotonin reuptake inhibitors (SSRIs) are prescribed off-label to delay ejaculation. These medications are typically antidepressants such as paroxetine (Paxil), sertraline (Zoloft), and fluoxetine (Prozac). Off-label means that these medications are prescribed for a purpose not officially approved by regulatory agencies such as the US Food and Drug Administration (FDA).
Medications such as these update the train’s brakes, adding more built-in resistance against the downward slope, and increasing the driver’s sense of control.
Pros:
- While it is off-label there is a well-researched evidence base that show these medications can significantly delay ejaculation.
- Generally low cost
- Does not require anticipating sexual activity
- Paroxetine (Paxil) shows the strongest ejaculatory delay compared to other off-label SSRIs
Cons:
- Not specifically approved for PE use
- Can have a larger risk of bodily side effects including fatigue, nausea, sweating, weight gain
- SSRIs are also known to cause other negative sexual side effects such as reduced libido, inability to orgasm, and erectile dysfunction
- Withdrawal symptoms can come with stopping the medication
- Relapse of PE is likely when medication is stopped
On-Demand Oral Medication:
These are medications consumed when anticipating intercourse. Unlike off-label prescriptions, the short acting SSRI dapoxetine (Priligy), was specifically licensed for PE. Tramadol (Ultram) is an off-label analgesic for PE that is refractory, meaning that it does not respond to standard or previous treatments.
Pros:
- Dapoxetine (Priligy) is effective on the first dose and is taken 1-3 hours before intercourse
- Reduces the chronic side effects associated with daily SSRIs
- Tramadol significantly improves ejaculation for PE that has not responded to other treatments
Cons:
- Requires the planning and anticipation of sexual activity
- Dapoxetine side effects may include nausea, dizziness, headaches, and diarrhea
- Tramadol requires careful patient monitoring due to risk of dependency and addiction
Combination Therapy:
Combining a medical approach with sex therapy is the optimal strategy especially when PE is lifelong or severe. This combination approach recognises that sexuality is a holistic experience, not just pure biology: there are significant psychological, relational, and even societal factors at play which influence sexual function.
Pros:
- Highest rates of sexual satisfaction in comparison to isolated treatments
- Increases treatment consistency
- Addresses biological factors and psychological and relational components
- Building lifelong skills to prevent relapse if and when medication is withdrawn
- Increases sexual confidence
Cons:
- There are financial costs, time, and commitment required by both medical and therapeutic approaches. Greater investment overall.
- Requires an actively supportive partner (when partnered)
Does Sex Therapy Help Premature Ejaculation?
While medical treatments can support the biological aspects of PE, sex therapy addresses the psychological, relational, and behavioural factors that often maintain the cycle.
In sex therapy, individuals learn to better understand their body’s patterns of arousal and excitement. Rather than the train racing up the hill uncontrollably, therapy focuses on developing awareness of the body’s signals earlier in the process. This allows space to slow the acceleration before the tipping point of ejaculatory inevitability is reached.
Sex therapy can support individuals to:
Build awareness of arousal levels and bodily cues
Reduce anxiety and performance pressure during sexual activity
Develop techniques to regulate pacing and stimulation
Rebuild sexual confidence
Expand sexual intimacy beyond the sole focus of penetration and ejaculation
When PE occurs within a relationship, couples sex therapy is often recommended. Premature ejaculation rarely affects only one person; both partners can experience frustration, disappointment, anxiety, or avoidance around sexual intimacy.
Couples therapy allows partners to approach the concern as a shared challenge rather than an individual problem. This helps reduce blame, strengthen communication, and rebuild a sense of teamwork in the sexual relationship.
Over time, many couples find that when pressure is reduced and communication improves, sexual intimacy becomes more relaxed and enjoyable for both partners.
Final Thoughts
Premature ejaculation can feel frustrating, embarrassing, and discouraging. Many delay seeking support out of shame or the belief that they should be able to “control it” on their own.
However, PE is both common and treatable. Effective treatment may involve behavioural strategies, medication, sex therapy, or a combination of these approaches. The right pathway will depend on the individual and relational factors involved.
Importantly, sexual satisfaction is not determined solely by how long intercourse lasts. When couples broaden their understanding of intimacy and reduce performance pressure, sexual experiences often become more pleasurable and connected overall.
If you are experiencing persistent concerns about premature ejaculation, speaking with your GP is an important first step.
I also offer online sex therapy across Australia, supporting individuals and couples navigating premature ejaculation and other sexual concerns. Together we can explore the factors involved, reduce performance pressure, and help you develop greater confidence and enjoyment in your sexual relationship.
Written by Justine
References
Waldinger MD. Problems of Ejaculation and Orgasm in the Male. In: Wylie K, editor. ABC of Sexual Health. 3rd ed. Chichester, UK: John Wiley & Sons Ltd; 2015. p. 73.
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, et al. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010;57(5):804-14.
Vukina J, McBride JA, Carson CC, Coward RM. Premature ejaculation. In: Dahm P, Dmochowski RR, editors. Evidence-Based Urology. 2nd ed. John Wiley & Sons Ltd; 2018. p. 569-77.
Betchen SJ. Premature Ejaculation: An Integrative, Intersystems Approach for Couples. J Fam Psychother. 2009;20(2-3):241-60.
Melnik T, Glina S, Rodrigues OM Jr. Psychological intervention for premature ejaculation. Nat Rev Urol. 2009;6(9):501-8.
Renshaw DC. Premature Ejaculation Revisited—2005. Fam J. 2005;13(2):150-2.
Rowland DL, Rose P. Understanding & Treating Premature Ejaculation. Nurse Pract. 2008;33(10):21-7.
American Psychiatric Association. Premature (Early) Ejaculation. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.